







Introduction
Menopause is a normal aging process and is defined as the absence of menstruation for 12 consecutive months (Moser et al., 2020). According to epidemiological studies, 60-68% of women experience menopausal symptoms at the beginning of menopause, and about 80% have symptoms such as flushing, night sweats, palpitations, dizziness, malaise, and hypersensitivity. There are serious symptoms that can affect you. Menopause can have a significant impact on health and quality of life, as women spend one-third of their lives after menopause (Bakhtiar et al., 2019). Menopause is characterized by follicular degeneration and ovarian estrogen secretion. In most menopausal women, estrogen deficiency causes HF, which manifests as hypothalamic thermoregulation (Rance et al., 2013). In the absence of estrogen, postmenopausal skin undergoes rapid intrinsic and extrinsic aging, resulting in wrinkles, thinning of the skin, and weakening of the cellular matrix (Holly et al., 2017). Hormone replacement therapy (HRT) has been the primary treatment for the management of menopausal symptoms, either as a combination of estrogen and progestogen or as estrogen alone. However, many menopausal women cannot or do not use HRT because of the health risks associated with it (Choi et al., 2018). Aromatherapy is a form of CAM that utilizes the healing properties of essential oils extracted from plants and is known to help maintain and promote physical and mental health. aromatherapy has been used in various ways such as massage, water bath, inhalation, foot bath, poultice, and cosmetics, and the particles of essential oils act on the limbic system of the brain through the sense of smell, skin, lungs, and circulatory will have psychological and physiological effects (Heo et al., 2016).
Therefore, the purpose of this study is to investigate whether aromatherapy as CAM is effective for HF and psychological anxiety, which are typical symptoms of middle-aged menopausal women, through a systematic review.
Materials and Methods
1. Search strategy
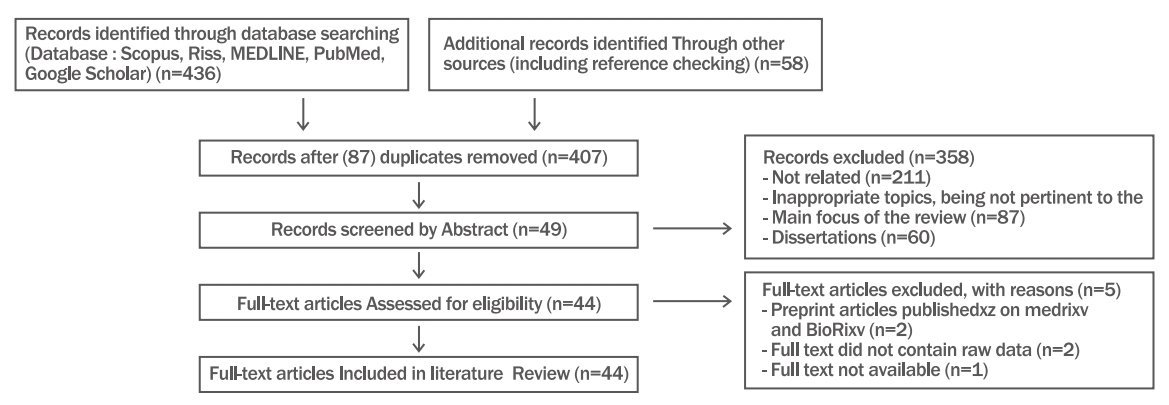
Although this literature review is a narrative review, we searched PubMed, Google Scholar, Scopus, and RISS, according to the PRISMA flow diagram guidelines, with the following search word chains: aromatherapy, menopause, hot flush, estrogen, complementary and alternative medicine. Figure1 illustrates the flowchart relating to the process of finding and selecting the studies included in this literature reviews.
2. Eligibility criteria
The articles included in this literature review had to meet the eligibility criteria of this literature review as follows. Studies on the effects of estrogen and aromatherapy on hot flashes in menopausal women were considered for inclusion. The effects of menopause on the skin, the role of estrogen in postmenopausal skin, and the use of aromatherapy for menopausal hot flashes.
3. Screening and data extraction
As inclusion criteria, we considered various article types, such as original research article, review article, internet article, brief report, and series. We did not apply restrictions on date of publication or language. The exclusion criteria were the following: full text not being accessible, full text not containing raw data, inappropriate topics, university thesis and dissertation, and not being pertinent to the main focus of the review.
4. Study selection and data extraction
This review is a critical literature review. In this study, a descriptive review approach was used. A total of 436 references were selected using representative journal search sites such as Pubmed, Google Scholar, Scopus, and RISS, using the PRISMA flow diagram. Accordingly, a total of 44 papers were selected in the final stage from 2000 to 2022. The PRISMA flowchart is shown in Figure 1. The model diagram of this study was organized as shown in Figure 2.
Findings
1. Effects of menopause on the skin
Hormonal changes during menopause can cause many side effects, along with physical, psychological, and sexual changes, and can affect a woman's life in a variety of ways (Nair, 2014). Menopause consists of a cessation of fertility in a woman's life cycle and is caused by a decrease in follicle activity. The ovaries are the main source of premenopausal estrogen production and are low levels of estrogen. As a result, hormonal changes have a particularly significant effect on the skin (Reus et al., 2020). The skin is the body's largest organ (Calleja-Agius & Brincat, 2012), a major barrier to the outside world, and plays an important role in controlling pathogens, controlling body temperature, and preventing desiccation (Elias, 2004). The skin is divided into the epidermis and dermis, with the exception of hair follicles, sebaceous glands, and sweat glands. The epidermis forms a thin outer layer of keratinocytes and melanocytes, and the dermis is a deeper layer. There is connective tissue between collagen and elastin (Calleja-Agius & Brincat, 2012). Menopausal symptoms appear quickly on the skin and tend to lose structural structure (Rzepecki et al., 2019). Many studies have shown that menopausal women detect early onset of skin aging symptoms (Thornton, 2013). The first symptom you experience is an increase in dryness of the skin followed by a decrease in elasticity. These symptoms are consistent with decreased sebum production and structural changes such as collagen content, dermis thickness, and elastin fibers (Rzepecki et al., 2019). About 80% of the dry weight of adult skin is made up of collagen, and collagen loss is a major cause of skin aging. Collagen fibers are placed flat on the surface of the skin and have high tensile strength on the skin. Prevents tearing due to expansion and contraction (Calleja-Agius & Brincat, 2012). Studies show that up to 30% of skin collagen can be lost in the first 5 years after menopause. It will decrease by about 2.1% per year (Sauerbronn et al., 2000). After menopause, the skin thins rapidly and the thickness of the postmenopausal skin decreases by 1.13% annually (Calleja-Agius et al,. 2013). Postmenopausal women's skin elasticity decreases by 0.55% each year after menopause, and facial skin aging is associated with a gradual increase in extensibility and a decrease in skin elasticity. Elastin makes up about 5% of the dermis and is involved in the elasticity of the skin. Elastin fibers are also produced by fibroblasts and placed in a thinly distributed subepithelial network. Connective tissue supports glycosaminoglycans (GAGs) and contains sensory receptors (Calleja-Agius & Brincat, 2012). Aged skin is characterized by a gradual decrease in skin thickness, primarily due to structural atrophic changes in the dermis. These changes include the loss of fibroblasts, resulting in reduced production of dermal collagen elastin and proteoglycan content (Archer, 2012), (Table 1).
2. The role of estrogen in postmenopausal skin
Estrogen is the most well-known hormone associated with menopausal symptoms (Davis et al., 2015). Estrogen depletion is associated with various metabolic mechanisms of aging, such as cell aging and oxidative stress (Labrie, 2015). Postmenopausal estrogen deficiency may explain accelerated skin aging, including decreased collagen and water content, decreased sebum secretion, and loss of elasticity (Calleja-Agius & Brincat, 2012). Estrogen targets keratinocytes, fibroblasts, melanocytes, hair follicles, and sebaceous glands to significantly regulate skin physiology and improve angiogenesis, wound healing, and immune response (Archer, 2012). A lack of estrogen reduces the defense against oxidative stress, thinning the skin by reducing collagen, reducing elasticity, increasing wrinkles, increasing dryness, and reducing blood vessels (Thornton, 2013). In the 1990s, researchers discovered that estrogen receptors are present in skin cells and their numbers decrease with the onset of menopause. Then estrogen Explored many ways to improve skin condition (Archer, 2012). Estrogen is a group of four steroid hormones, including estrone, 17β-estradiol, estriol, and estetrol, and most of the physiological roles associated with estrogen are related to 17β–estradiol (Shu & Maibach, 2011). Postmenopausal 17β-estradiol loss is an important cause of tissue aging in women (Wilkinson & Hardman, 2017). In women of childbearing age, estrogen biosynthesis occurs primarily in the ovaries, and after menopause, aromatase activity in peripheral areas such as the skin converts DHEA (dihydroepiandrosterone) to estrogen (Wilkinson & Hardman, 2020). A deficiency of 17β-estradiol in postmenopausal skin causes sweat and sebaceous glands to function poorly, leaving the skin dehydrated and dry (Zouboulis & Boschnakow, 2001). In the absence of estrogen (17β-estradiol), postmenopausal skin ages rapidly, causing wrinkles, thinning of the skin, and weakening of the extracellular matrix (Posadzki et al., 2013). HTR is the primary treatment for menopausal symptoms, but many women are unable or unwilling to use it because of the health risks associated with it (Johnson et al., 2019). 50% of postmenopausal women use CAM, and more than 60% recognize that CAM is effective for menopausal symptoms (Posadzki et al., 2013).
Therefore, various CAMs that can relieve menopausal symptoms are needed. Non-hormonal substances such as phytoestrogens as a safe remedy are becoming more and more interesting to postmenopausal women (Saghafi et al., 2017). Phytoestrogens are non-steroidal plant-derived compounds derived from various herbs that can cause estrogenic effects (Lin et al., 2017). Phytoestrogens reduce the frequency and intensity of HF without side effects (Chen et al., 2015). As the effectiveness of various herbs on vasomotor and psychogenic symptoms of menopause has been observed in various studies, there are increasing reports that plants containing phytoestrogens are particularly effective in alleviating the symptoms (Kargozar et al., 2017). Many other plant-derived sera or phytoestrogens have positive effects on skin aging, including protection from oxidative damage and restoration of skin moisture and collagen content (Liu et al., 2020), (Table 2).
3. Effects of aromatherapy on menopausal HF
HF are the most common complaint among women experiencing menopause (Umland, 2008). HF have a significant impact on quality of life, but are often underestimated. HF interfere with activities of daily living and sleep, causing fatigue, loss of concentration, and depression. All of these can cause problems in family life (Strudee, 2008). HF are a major menopausal symptom that more than 80% of menopausal women experience and want to seek treatment (Thurston & Joffe, 2011). The strength of HF. Frequency, severity, and duration vary from person to person, and a Women's Health Across the Nation (SWAN) survey of 16,000 women found that some women experienced monthly or weekly HF. But in other women, it happened frequently every day (Bromberger et al, 2007). HF are reported as a high fever with chills and usually appear on the face, neck, and chest. In one study in the United States, 87% of women reported HF every day, and one-third reported experiencing more than 10 HF per day (Freedman, 2014). The ovaries, which lower the levels of estrogen in the blood circulation, increase the activity and stimulation of upper and lower serotonin receptors. Activation of these receptors promotes changes in the thermoregulatory center, stimulates autonomic responses such as elevated body temperature and sweating, and causes HF (Kazemzadeh et al., 2016).
The main treatment for HF is HRT, which can reduce it by 70-80% (Albertazzi, 2006). HF are estrogen-related because they occur in the majority of women with spontaneous or surgical menopause, which is consistent with the fact that estrogen therapy actually eliminates HF (Freedman, 2014). However, more patients are considering non-hormone therapy because certain side effects of HRT increase the risk of breast cancer, thrombophlebitis, hypertension, vaginal bleeding, and bile sac disease (Taghizadeh et al., 2006). Several studies have shown that aromatherapy reduces the frequency of HF during menopause. Inhalation of lavender scent for 20 minutes, twice a day for 12 weeks in 100 menopausal women aged 45 to 55 years, improved HF (Kazemzadeh et al., 2016).
In another study, inhalation of 2% lavender essential oil for 20 minutes before bedtime each night improved HF in 62 postmenopausal women (Bakhtiar et al., 2019). Diluted almond oil (90%) and evening primrose oil (10%) using aromatic oils such as lavender, rose geranium, rose, and rosemary in a ratio of 4:2:1:1 at the menopausal clinic of the obstetrics and gynecology hospital to a final concentration of 3 %, and received 30-minute massage treatment twice a week for 4 weeks, and there was an effect of improving HF (Fatemeh et al., 2012). A study of inhaled lavender in postmenopausal women suffering from hot flashes found that hot flashes were reduced, not only hot flashes, but also anxiety, depression, physical and vasomotor symptoms (Nikjou et al., 2018), (Table 3).
4. Positive prospects for aromatherapy effects
Aromatherapy has long been used to improve women's health (Tillett & Ames, 2010). Aromatherapy is one of the oldest CAMs in which essential oils extracted from plants are applied in a variety of ways, including inhalation, oral cavity, bathing and massage (Taavoni et al., 2013). The fragrance inhalation method spreads throughout the body by breathing, so the essential oil components are detected in the blood within 5 minutes after inhalation and act directly on the brain within 20 minutes, so the effect is very good (Jung & Song, 2018). The mechanism of the aromatherapy effect involves the uptake of essential oils into the biological signals of nasal receptor cells during inhalation, which are transmitted via the olfactory bulb to the marginal and hypothalamic systems of the brain. These signals trigger the brain to release neurotransmitters such as serotonin and endorphins, allowing the nervous system and other nervous systems to connect and feel comfortable with the desired changes (Salehi-Pourmehr et al., 2020). Aromatherapy has few side effects and is effective in menopause control, anxiety control, obesity control, stress control, depression control, sleep control, pain control, fatigue control, and blood pressure control. It is known that there is strengthening effect (Heo et al., 2016). With the development of complementary and alternative medicine, scientific research on the effects of aromatherapy is being conducted from various angles (Toda & Morimoto, 2008). Aromatherapy is a method for solving menopausal symptoms, psychological, physical and social problems in middle-aged women. Studies have been published reporting the effects of applying various essential oil techniques (Heidari, 2017). aromatherapy is effective in significantly relieving menopausal symptoms in middle-aged women and may improve the health and well-being of menopausal women (Table 4).
Conclusions
In the course of this study, it was found that aromatherapy is effective for HF in menopausal middle-aged women. Menopause and skin quality are closely related. HF are the most characteristic and major symptom of menopause and do not pose a threat to women's health, but reduce their quality of life. Estrogen deficiency, the main cause of redness, accelerates skin aging such as dryness, atrophy and fine lines. As the population of menopausal women continues to increase, aromatherapy for menopausal middle-aged women who cannot use HRT or suffer from unwanted HR is the simplest, non-invasive, safe and effective method that can be used anytime, anywhere, regardless of location. It seems to be one of CAM.
However, detailed information on the pharmacological or causal relationship to aroma oil is lacking, so more systematic and diverse studies are needed.